The problems of missing and ectopic second bicuspids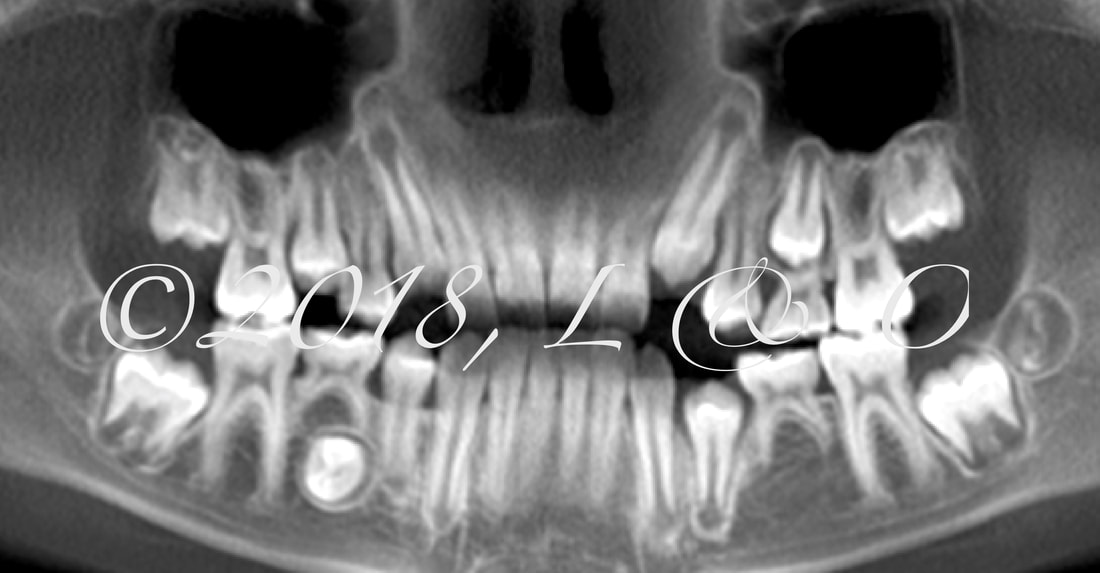 Severely ectopic LR5 had to be removed. © 2018
0 Comments
Relationships are transformational for your dental practice. Deal with your patients with absolute love in your heart. "If words come out of the heart, they will enter the heart. If they come from the tongue, they will not pass beyond the ears." - Suhrawardi
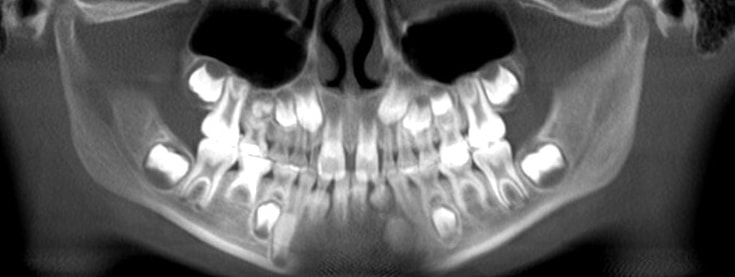 Missing upper 2's, missing lower 5's, ectopic canines. © 2018 Dr Chris Baker The Panoramic radiograph. You may be surprised to discover the amazing information you can find about a child patient in that x-ray. Can you name five really important findings in a panoramic on an early mixed dentition patient? Can you name six? Seven? Let’s go for double that figure! (And we won’t include decay, as it’s not the best diagnostic tool of decay. Well, on second thought, maybe we will include some possible decay-related findings at the end of our discussion.) The panoramic should be taken when any permanent teeth are erupting. Often those first eruptions are the lower incisors, or the six-year molars, but no matter what teeth, take the pano then. (You may find opportunity to change the child’s life because of the secrets that x-ray holds.) Start by counting/identifying all teeth (Sounds pretty tame and familiar so far!) :
Here’s an important opportunity to do outstanding diagnosis for your patient, and be paid for your care. You’re in dentistry to care for people, and in business to make a living.  Missing LL5, and severely ectopic LR 5, which had to be removed. © 2018 Dr Chris Baker
Using the right systems is the "secret sauce" to successfully implement an orthodontic program in a general or pediatric dental practice.
 Some of the past officers of the American Orthodontic Society. Past President, Dr Chris Baker, is on the very right. Some of the past officers of the American Orthodontic Society. Past President, Dr Chris Baker, is on the very right. Choose freedom over paying some corporate CEO’s country club membership...
Benjamin Franklin warned of the kind of situation where little compromises sacrifice such freedoms; “Make yourself a sheep and the wolves will eat you.” Opt into a free market medical model - and YOU decide what your missionary work will be instead of being a member of the unpaid robot dental collective. Dr. David Gesko, in a recent interview, notes, if you're concerned about dental therapists from a competition standpoint, dentistry as a whole is changing, and you may have to get used to new technologies and models of care. (emphasis mine)1 Choose freedom over being required to change your “model of care” (How about if you go out of business, and two dental therapists with high school educations replace you?) Use a free market model, instead, that makes you independent of big insurance, big government and big corporations. It seems the biggest advocates for cheaper dental (medical) care are executives of huge corporations, receiving very generous salaries. The young dentist out of school with a half-million dollar debt needs his/her profession, his/her job, his/her ability to proceed with a career, take care of a beloved family and get out of debt. Dr Gesko is Dental Director and Senior Vice-President of HealthPartners, a corporation which reports “serving over 1.5 million members.” 2 His biography says, “Dr. Gesko is passionate about integrating medical and dental care and applying growing evidence-based research to care delivery.” (emphasis mine)2 Dr. Gesko, a Minnesota Board of Dentistry member, and now President of the Board, says he has worked alongside dental therapists since their inception. So far, he's had “positive experiences and so have the low-income patients at HealthPartners' dental clinics.”1 Use a model to create a life where you are free, prosperous, and happy. You can use situations and systems which, if implemented, will give you the interesting, wonderful, and prosperous practice you deserve. You can take better care of your patients, family, staff, and be a better member of the community, by implementing the systems we teach. At Love & Orthodontics, we are here to help the dentist have the practice of his/her dream. You, the dentist can have a happy career that is prosperous and free of harassment from insurance companies, big corporations and government over-regulation. Fear knocked at the door Faith answered. No one was there. 1. https://www.drbicuspid.com/index.aspx?sec=sup&sub=pmt&pag=dis&ItemID=323014 2. http://www.marshfieldresearch.org/iosh/biography-of-david-gesko The best treatment of the patient, doctor, is still YOUR responsibility.
 An idea. Carve out dinner times as often as possible, to be together. To be at peace. To share your day. To enjoy each other. We need to become aware of studies that show us that children are being damaged by screens and by the content on those screens and of studies about the high risk of cancer from screen use. And, of the breakdown of families and the terrible impact on all. SO - picture dinner times as often as possible, together as a family, all devices out of the room, and talk and sharing with the food. Even include preparation of the food. How about making a delicious soup, and serving it with a healthful toast? Here’s a wonderful, easy, quick recipe that could be fun for you all to make: Yummy Butternut Squash Soup - makes about 4-5 servings • about 8 cups of fresh cubed butternut squash, which you can find in the produce section of most groceries; • Olive Oil; • about 20 oz. of vegetable or chicken broth; • about 2 c Heavy Cream; • A large bag of baby spinach and a large chopped onion to saute to serve with your soup; • Creme fraiche or sour cream or yogurt. Preheat oven to 350 degrees. Turn squash cubes in oil until well coated. Put onto baking sheet or baking pan, single layer, and roast at 400 deg for about an hour, until they are brown on the edges. Can refrigerate at this point until ready to make the soup. Blitz squash with broth in processor or with stick blender, and heat through. Add cream Saute chopped onion in olive oil, remove, then a bit more olive oil, and dump your large bag of spinach into the saute pan and saute til wilted. Serve your soup as you wish - top with your sautéed spinach and onion, creme fraiche, sour cream or yogurt, and. and sprinkle with red chili flakes if you want a touch of spicy, Yum. Love,
So, the result is the trend away from the customary, conventional, standard restorative treatments, and toward “minimally invasive” and even “non-invasive” treatments. These fashionable offerings basically ignore the bacterial etiology of dental decay and soft tissue inflammation and infection, with a nod to making it easier, more acceptable to the child, and thus to the parent. Certainly those of us who treat children have experienced the question, "Johnnie, do you want to have your tooth fixed today? (Variations; “pulled", "pulled out", "numbed", "have a shot," etc.) What child would not answer, “No”? We could go into the point that’s why children have parents, to make the difficult decisions that will most benefit their children, but even that point is not the point here. So, it is becoming de rigueur to treatment plan the more acceptable treatments that do not address the bacterial etiology - hear me - as well - and keep everyone happy. Even our “evidence base” finds the Hall SSC technique of covering a decayed tooth with an SSC (often without any decay removal) as acceptable. So the virulent organisms are locked into the tooth where they can travel through dentinal tubules into the pulpal circulation and into the systemic circulation. My job is not to judge the research, nor the treatment, but to have you consider - and question - what the sequelae to these directions may be. "Minimally invasive” techniques include diet counseling and sugar substitutes, sealants, antimicrobial agents and chemotherapeutic approaches, remineralization of early lesions, GIC, fluorides, CPP-ACP, and others. Let’s think about those first. Have you many parents in your practice who truly take the information to heart and... a) change the child’s diet , b) actually use the antimicrobial agents, fluorides, and other chemotherapeutic agents over even a short period of time, and regularly? It begs the question, “How’s it workin’ for ya?” Then the minimal surgical interventions of decay, including ART, chemo-mechanical caries removal (Sodium hypochlorite + mechanical removal), air abrasion, lasers, Hall technique, Silver Diamine Fl, and so on - while these are newer on the scene, how do you feel those approaches transform the child’s history and future of decay? (An attorney in my family responded that on behalf of all attorneys, he might just mail a thank you note to Dr. Hall, whoever he is, for his technique that makes it just a matter of time before he earns a very good living for attorneys.) It’s the “How’s it workin’ for ya?” again. HOWEVER, we as pediatric dentists LOVE to please the parent and child. Most folks who go into dentistry are... a) in it to help people and change lives, and... b) approval addicted such that it is a common goal to do whatever possible to get people to LOVE you. (That includes not charging either anything for some procedures, or at least not much, not “bothering the child patient if possible, using GA, sedation, etc.) So, these less invasive, hated treatments appeal to us as well as to the parents and child. Sort of. We convince ourselves it is good. That train is carrying other cargo as well. Think about:
~ Johnny Cash Doctor, are you dancin’ on the tracks?
|

Dr Chris BakerAmerica's most-trusted teacher of orthodontic continuing education, Dr. Chris Baker has practiced and taught for more than 30 years, and is a current or former faculty member of three U.S. dental schools. She is a pediatric dentist, author, blogger, dental practice consultant, and mentor. Dr. Chris is also Past President and Senior Instructor of the American Orthodontic Society. She is based in Texas, USA, but lectures around the world. Categories
All
Archives
July 2024
Text and images
© 2024 Dr Chris Baker |








 RSS Feed
RSS Feed